
What is Pneumonia
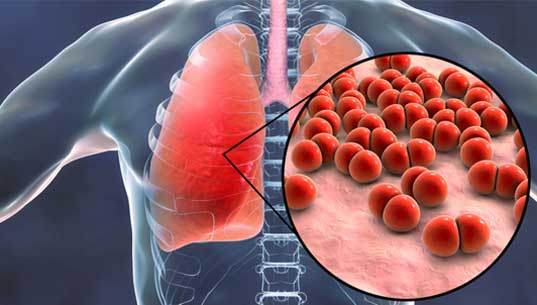
Pneumonia is an infection of the lungs with a range of possible causes. It can be a serious and life-threatening disease. It normally starts with a bacterial, viral, or fungal infection.
The lungs become inflamed, and the tiny air sacs, or alveoli, inside the lungs fill up with fluid.
Here are some key points about this disease. More detail is in the main article.
- Pneumonia is an infection of the lungs that can cause mild to severe illness in people of all ages.
- It is the one of the leading causes of hospital admissions and death worldwide
- Those at high risk for this disease include older adults, the very young, and people with underlying health problems.
Risk for Pneumonia
Those most at risk include people who:
- Are over 65 years
- Smoke tobacco, consume large amounts of alcohol, or both
- have underlying conditions such as cystic fibrosis, chronic obstructive pulmonary disorder (COPD), asthma, or conditions that affect the kidneys, heart, or liver
- have a weakened or impaired immune system for example due to HIV or cancer
- Being on medications which suppress immune system
- Organ transplant or bone marrow transplant recipients
- have recently recovered from a cold or influenza infection
- experience malnutrition
- have been recently hospitalized in an intensive care unit
- have been exposed to certain chemicals or pollutants
Prevention
There are two different vaccines to prevent this disease, the most common bacterial cause of pneumonia.
These cover a wide variety of pneumococcal infections
- Pneumococcal conjugate vaccine, or Prevnar
- Pneumococcal polysaccharide vaccine, or Pneumovax
Diagnosis
A doctor will ask about symptoms and medical history and will carry out a physical examination.
They may suspect pneumonia if they hear coarse breathing, wheezing, crackling, or decreased breath sounds when listening to the chest through a stethoscope. The doctor may also check the oxygen levels in the blood with a painless monitor on the finger called a pulse oximeter.
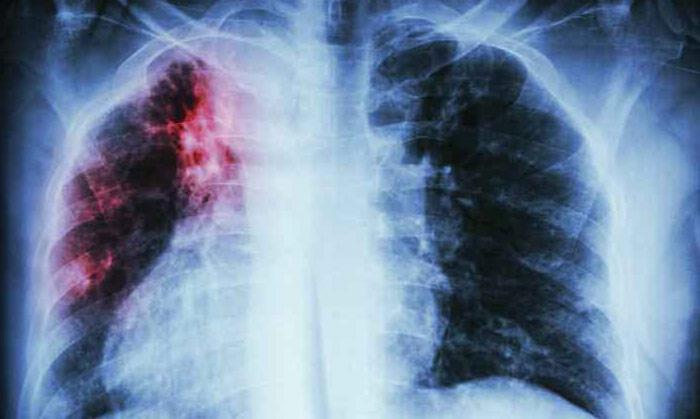
- Chest X-rays
- CT scan
- Blood tests
- Blood cultures
- An arterial blood gas (ABG)
- A sputum analysis
Treatment of Pneumonia
Treatment depends on the type and severity of pneumonia.
- Bacterial types of pneumonia are usually treated with antibiotics.
- Viral types of pneumonia are usually treated with rest and plenty of fluids. Antiviral medications can be used in influenza.
- Fungal types of pneumonia are usually treated with antifungal medications.
Doctors can provide treatment which include treatments for reducing fever, treating infection and inflammation . Dr. Anand Singh is a pneumonia specialist doctor in The Clementine Churchill Hospital in Harrow, and Syon Clinic in Brentford, West London, OSD Healthcare Hertfordshire.
● ABOUT DR ANAND SINGH
About Dr Anand Singh
Dr Anand Singh is a highly experienced Consultant Respiratory Physician with over a decade of experience in the field.
Dr Singh is a well known Chest Consultant and Sleep Consultant who provides personalised treatment plan.
Dr Anand Singh is a consultant Respiratory Physician at West Hertfordshire Teaching Hospitals NHS Trust
(Watford General and Hemel Hempstead Hospital where he leads the Sleep and Non-Invasive ventilation Service
and Respiratory High Dependency unit. He undertakes sub-speciality clinics in Interstitial Lung diseases
and Sleep Apnoea as well as conducting general respiratory medicine clinics.
Professional Memberships


Recommended by patients
Interstitial Lung Disease (ILD)
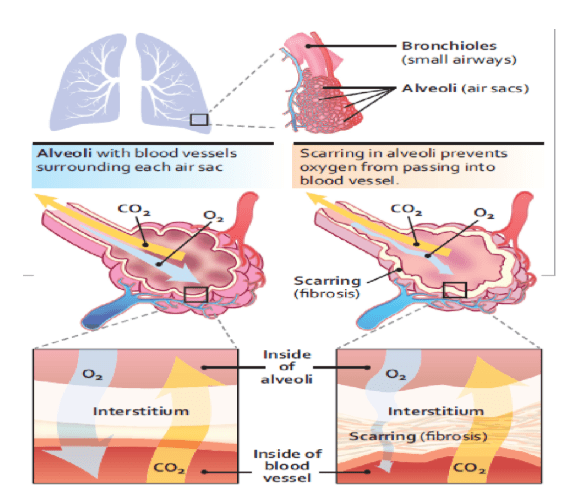
Interstitial lung disease describes a large group of disorders, most of which cause progressive scarring of lung tissue. The scarring associated with interstitial lung disease eventually affects your ability to breathe and get enough oxygen into your bloodstream. Interstitial lung disease describes a large group of disorders, most of which cause progressive scarring of lung tissue. The scarring associated with interstitial lung disease eventually affects your ability to breathe and get enough oxygen into your bloodstream. Dr. Anand Singh provides treatment for all interstitial lung diseases.
This disease can be caused by long-term exposure to hazardous materials, such as asbestos. Some types of autoimmune diseases, such as rheumatoid arthritis, also can cause ILD. In some cases, however, the causes remain unknown.
Some types of lung scarring can be reversible if picked up early and treated and the causative factor is removed.
“For many types of lung scarring , it’s generally irreversible”, Says Dr. Anand Singh, Lung specialists in The Clementine Churchill Hospital in Harrow, and Syon Clinic in Brentford, West London, OSD Healthcare Hertfordshire. Medications may slow the damage of this disease, but many people never regain full use of their lungs.
For any diseases causing progressive scarring of lung treatment by an lung specialists should be done.
Dr. Anand Singh is an expert Lung specialists in The Clementine Churchill Hospital in Harrow, and Syon Clinic in Brentford, West London, OSD Healthcare Hertfordshire with experience in managing all interstitial and fibrotic lung diseases
Lung transplant is an option for some people who have ILD.
Cause of ILD
This disease seems to occur when an injury to your lungs triggers an abnormal healing response. Ordinarily, your body generates just the right amount of tissue to repair the damage. But in ILD, the repair process goes awry and the tissue around the air sacs (alveoli) becomes scarred and thickened. This makes it more difficult for oxygen to pass into your bloodstream. Occupational and environmental factors
- Silica dust
- Asbestos fibers
- Grain dust
- Bird and animal droppings
- Radiation treatments
- Indoor hot tubs
Factors that may make you more susceptible to interstitial lung disease include:
- Age: ILD is much more likely to affect adults, although children sometimes develop the disorder.
- Exposure to occupational and environmental toxins: If you work in mining, farming or construction or for any reason are exposed to pollutants known to damage your lungs, your risk of interstitial lung disease is increased.
- Gastroesophageal reflux disease: If you have uncontrolled acid reflux or indigestion, you may be at increased risk of this disease.
- Smoking: Some forms of ILD are more likely to occur in people with a history of smoking, and active smoking may make the condition worse, especially if there is associated emphysema.
- Radiation and chemotherapy: Having radiation treatments to your chest or using some chemotherapy drugs make it more likely that you’ll develop lung disease.
Interstitial Lung Disease Prevention
There is no way to prevent idiopathic or genetic ILD, but it is possible to prevent some of the types with known causes. You can reduce your risk by:
- Wearing a respirator (a mask that filters particles from the air) around harmful substances, such as asbestos, metal dust, or chemicals.
- Quitting smoking.
- Receiving immunizations for flu and pneumonia to help protect your lungs.
Diagnosis Of Interstitial Lung Disease
Identifying and determining the cause of ILD can be challenging. A large number of disorders fall into this broad category. In addition, the signs and symptoms of a wide range of medical conditions can mimic interstitial lung disease, and doctors must rule these out before making a definitive diagnosis.
Some of the following tests may be necessary.
- Blood tests
- Computerized tomography (CT) scan.
- Echocardiogram
- Pulmonary function tests
- Bronchoscopy
- Lung tissue analysis
Treatment of Interstitial Lung Disease
The lung scarring that occurs in many subtypes of this disease can’t be reversed, and treatment will not always be effective in stopping the ultimate progression of the disease. Some treatments may improve symptoms temporarily or slow the disease’s progress. Others help improve the quality of life.
Dr. Anand Singh – Lung specialist in The Clementine Churchill Hospital in Harrow, and Syon Clinic in Brentford, West London, OSD Healthcare Hertfordshire is of the opinion that early diagnosis , treatment initiation and removal of causative factor ( if applicable is important)
Medications
Intense research to identify treatment options for specific types of interstitial lung disease is ongoing. Based on currently available, scientific evidence, however, your doctor may recommend:
- Corticosteroid medications.
- Medications that slow the progression of idiopathic pulmonary fibrosis like Anti fibrotics
- Immunosuppressive medications
- Medications that reduce stomach acid.
- Oxygen therapy
- Pulmonary rehabilitation
● ABOUT DR ANAND SINGH
About Dr Anand Singh
Dr Anand Singh is a highly experienced Consultant Respiratory Physician with over a decade of experience in the field.
Dr Singh is a well known Chest Consultant and Sleep Consultant who provides personalised treatment plan.
Dr Anand Singh is a consultant Respiratory Physician at West Hertfordshire Teaching Hospitals NHS Trust
(Watford General and Hemel Hempstead Hospital where he leads the Sleep and Non-Invasive ventilation Service
and Respiratory High Dependency unit. He undertakes sub-speciality clinics in Interstitial Lung diseases
and Sleep Apnoea as well as conducting general respiratory medicine clinics.
Professional Memberships
Recommended by patients
What is Pleural Diseases?
The pleura is the membrane that lines the thoracic cavity and covers the lungs. The layers of the pleura contain a small amount of fluid that acts as a lubricant as one breathes in and out. The space between the layers is called the pleural cavity.
Types of Pleural Diseases
- Pleural effusion: This is excess fluid in the pleural cavity. This is one of the most common problems associated with the pleura. The most common cause is congestive heart failure. Other causes include lung cancer, pneumonia, tuberculosis, liver disease, pulmonary embolism.
- Hemothorax: is a buildup of blood in the pleural cavity. Chest trauma due to the accident is the most common cause, but cancer of the lung or pleura or open-heart surgery can also cause a hemothorax.
- Empyema: The accumulation of pus in the pleural cavity. This is a type of pleural effusion that is usually associated with pneumonia. The symptoms are those of pneumonia (cough, fever) in addition to shortness of breath and impaired breathing.
- Pleural tumours: Pleural tumours are cancerous tissues in the pleural cavity. This can be a Mesothelioma . Alternately pleural tumours may be cancers that have spread from other areas of the body. Symptoms: Shortness of breath, chest pain, cough, unexpected weight loss
- Pleurisy is pain associated with inflammation of the pleural cavity. The most common cause is a viral infection, such as influenza. Other causes include bacterial and fungal infections, lung cancer, other diseases such as rheumatoid arthritis. Symptoms of pleurisy may include a sharp pain when breathing, shortness of breath, a cough, fever and chills, rapid breathing, unexplained weight loss, and sore throat followed by joint swelling and soreness.
- Pneumothorax: Pneumothorax is a buildup of air or gas in the pleural cavity around the lung that causes the lung to collapse. Chronic obstructive pulmonary disease, tuberculosis, and trauma are the most common causes. Symptoms: Shortness of breath, rapid breathing, chest pain when taking a deep breath (pleurisy), cyanosis (bluish discoloration of the skin), respiratory distress can occur.
Diagnosis
This disease may be suspected on the basis of medical history and findings on a physical examination.
It is confirmed with a chest x-ray, which shows the interior of the chest cavity, and a CT scan—a series of images of the inside of the body, taken from different angles and depths, to reveal a high level of detail. Pleural Ultrasound is an important diagnostic tool.
To ensure that the blood vessels and organs show up clearly in these scans, the dye may be injected into a vein during the performance of the scan. Certain blood tests may also be useful in determining the cause and severity of this disease.
Treatment of Pleural Diseases
The treatment of this disease is dictated by the condition and may vary from
Placement of a chest tube to evacuate air
- Thoracentesis: draining fluid with a needle or a chest tube
- Decortication: Opening the chest to remove the diseased pleura
- Video-Assisted Thoracoscopic Surgery (VATS): Treatment for mechanical problems (fluid, air, or blood) focuses mainly on removing the fluid, air, or blood A minimally invasive alternative to open-chest surgery that involves less pain and recovery time. After you receive a sedative, your surgeon will make tiny incisions in your chest and then insert a fiber-optic camera called a thoracoscope. Images from the thoracoscope will give the pulmonologist important information that will help guide the appropriate treatment.
- Abrading the pleural surface / Pleurodesis to achieve adherence to the lung to the chest wall may be required for recurrent pneumothorax.
- Extrapleural pneumonectomy: In some cases of malignancy (mesothelioma), removal of all of the pleura, as well as the underlying lung, may be indicated after multidiscilipinary involvement with oncologist and Thoracic Surgeon.
● ABOUT DR ANAND SINGH
About Dr Anand Singh
Dr Anand Singh is a highly experienced Consultant Respiratory Physician with over a decade of experience in the field.
Dr Singh is a well known Chest Consultant and Sleep Consultant who provides personalised treatment plan.
Dr Anand Singh is a consultant Respiratory Physician at West Hertfordshire Teaching Hospitals NHS Trust
(Watford General and Hemel Hempstead Hospital where he leads the Sleep and Non-Invasive ventilation Service
and Respiratory High Dependency unit. He undertakes sub-speciality clinics in Interstitial Lung diseases
and Sleep Apnoea as well as conducting general respiratory medicine clinics.
Professional Memberships
Recommended by patients
What Is Obstructive Sleep Apnea in Adults?
Obstructive sleep apnea (OSA) is a common problem that affects a person’s breathing during sleep. A person with OSA has times during sleep in which air cannot flow normally into the lungs. The block in airflow (obstruction) is usually caused by the collapse of the soft tissues in the back of the throat (upper airway) and tongue during sleep.
Apnea means not breathing. In OSA, you may stop breathing for short periods of time. Even when you are trying to breathe, there may be little or no airflow into the lungs. These pauses in airflow (obstructive apneas) can occur off and on during sleep, and cause you to wake up from a sound sleep. Frequent apneas can cause many problems. With time, if not treated, serious health problems may develop.
OSA is more common in men . Treatment for OSA should always be under the guidance of a sleep specialist doctor or Obstructive sleep apnea specialist doctor. People who are at higher risk of developing sleep apnea include those with:
- Enlarged tonsils and/or adenoids
- Cardiac / heart issues
- Increased neck circumference
- Smokers
- Family history of OSA
- Excessive weight / high body mass index
- Jaw problems such as micrognathia (small jaw) or retrognathia (a pulled back jaw)
- Consuming Alcohol
Growing Awareness About Effective Care
As more patients seek reliable solutions, many are turning to evidence-based options such as sleep apnea treatment in London, especially when traveling or staying abroad. Increased global awareness is helping adults understand the importance of early diagnosis and professional assessment when symptoms first appear.
What are the symptoms of obstructive sleep apnea?
You may not be aware that you have OSA, but these symptoms may be more obvious to a spouse, another family member, or close friend.
Common symptoms you may have during sleep:
- Snoring is usually loud and bothers other people trying to sleep near you. Snoring can come and go through the night.
- Gasping or choking sounds.
- Breathing pauses observed by someone watching you sleep.
- Sudden or jerky body movements.
- Restless tossing and turning.
- Frequent awakenings from sleep.
Common symptoms you may have while awake:
- Wake up feeling like you have not had enough sleep, even after sleeping many hours.
- Morning headache.
- Dry or sore throat in the morning from breathing through your mouth during sleep.
- Sleepiness during the day.
- Fatigue or tiredness throughout the day.
- Personality changes, such as mood swings and difficulty getting along with others.
- Problems with poor memory or inability to concentrate.
Can OSA be dangerous?
Of all people with hypertension, about 30% have obstructive sleep apnea. If you have obstructive sleep apnea, there is a higher chance you also have hypertension.
Problems with the rhythm of your heart may occur with OSA such as atrial fibrillation (a type of irregular heartbeat) and bradycardia (slow heart rate). People with severe obstructive sleep apnea are more likely to have atrial fibrillation compared to those without OSA.
What kinds of cardiovascular problems can I get with obstructive sleep apnea?
Of all people with hypertension, over 30% have obstructive sleep apnea. If you have obstructive sleep apnea, there is a 50% chance you also have hypertension.
Problems with the rhythm of your heart may occur with OSA such as atrial fibrillation (a type of irregular heartbeat) and bradycardia (slow heart rate). People with severe obstructive sleep apnea are four times more likely to have atrial fibrillation compared to those without OSA.
People with obstructive sleep apnea are also more likely to have coronary artery disease. Coronary artery disease (also known as the hardening of the arteries) happens when the small blood vessels that supply blood and oxygen to your heart become narrow. Narrowed coronary arteries can lead to heart attacks and heart damage. If you have severe OSA that is untreated, you are twice as likely to develop a heart attack in the future as those without OSA. In addition, research shows that up to 70% of people admitted to the hospital because of coronary artery disease were found to have obstructive sleep apnea.
If you have heart failure, obstructive sleep apnea can also make it worse.
When to Seek Professional Guidance
Early evaluation is essential for accurate diagnosis and timely care. Many individuals traveling frequently are choosing reputable services such as sleep apnea treatment in London, ensuring they do not delay critical assessments even while away from home. Accessing professional support can prevent long-term complications.
How do I know I have OSA?
If you have symptoms of OSA, you need to talk with your healthcare provider. Your healthcare provider can help you decide if you need a sleep study and whether you should be evaluated further at a sleep center.
Dr. Anand Singh – Obstructive sleep apnea specialist doctor would do a sleep study for its detection. During a sleep study, your breathing, heart rate, and oxygen levels will be monitored.
How is obstructive sleep apnea treated?
Sleep apnea can be effectively treated, and there are a number of ways to do so. The choice of treatment will depend on the reason for and severity of the sleep apnea. If your OSA is from being overweight, weight loss may cause the apnea to go away completely.
Cpap Machine is usually the most effective and evidence based approach to treat Sleep Apnea.
As alcohol can suppress breathing and make OSA worse, avoid alcohol for at least 4 hours before going to bed. Sleep apnea is often worse when a person sleeps on his or her back. If you sleep on your back, you can use a pillow or some other strategy to force yourself to sleep on your side. Mandible splint devices are generally less effective for OSA and are meant for only mild cases . These devices are usually custom-made and fitted under the supervision of a specialized dentist or oral surgeon who works with these problems. They are less effective at reducing cardiovascular risks than a Cpap machine.
Surgery may also be helpful for people with jaw problems. Other surgeries for OSA either clear out a tissue from the back of the throat, reposition the tongue forward. These surgeries are not, however, as effective as CPAP to control OSA and are usually reserved for people who fail CPAP.
Hypoglossal nerve stimulation (HGNS) uses a pacemaker-like stimulator device that a surgeon places in the neck and use electricity to activate the muscles in the tongue to hold the airway open. HGNS recently received approval by the Food and Drug Administration (FDA) and is being used increasingly in the past year
Will my OSA ever go away?
In general, OSA is considered a lifelong condition, although there are few exceptions in which OSA can improve or go away. Obesity is a major risk factor for OSA and weight loss has been shown to lead to an improvement in OSA. Stomach stapling (bariatric surgery) can be highly effective for losing weight, although as with any surgery, complications can occasionally occur. The other situation in which apnea can resolve is in people with large tonsils that are blocking airflow in the throat. Removal of tonsils, particularly in children, has been shown to improve OSA. However, the removal of tonsils is typically not sufficient to treat OSA in adults.
Why should I wear CPAP at night?
Dr. Anand Singh – Obstructive sleep apnea specialist notes three major benefits of using CPAP with sleep:
■ Snoring is often annoying to the bed partner, such that many people with sleep apnea use CPAP to keep their partner happy. Some people think snoring is funny or a nuisance, but it can have a big impact on the quality of life if it interferes with intimacy or disrupts the sleep of the bed partner.
■ CPAP can improve symptoms. Many people feel better after using nocturnal CPAP they have a new lease of life. Research trials have shown improved daytime sleepiness, quality of life, and reduced risk of car accidents.
■ CPAP can improve cardiac and diabetes risk. CPAP has been shown in research trials to improve high blood pressure and likely reduces the risk of heart attack and other serious medical conditions.
What happens if I can’t tolerate CPAP therapy?
CPAP therapy can provide major benefits for most patients but it is not for everyone. OSA specialist doctors Most sleep experts will recommend further attempts of a different type of positive airway pressure therapy for patients who don’t like CPAP. A variety of masks and pressure delivery approaches are available so patients are encouraged to try various devices before giving up. Education and support can also be helpful in getting people used to using the CPAP machine. Sometimes psychologists or respiratory therapists can be helpful in getting you to get used to the equipment and being able to sleep with the equipment on. CPAP can be uncomfortable when you are not used to it but so many patients do well if they stick with it over time.
Lifestyle measures , sleep hygiene measures are encouraged and you can discuss further options for a customised plan .
Weight loss jabs may be considered after consulting your Primary care doctor / General practitioner .
Call to Action: Take Control of Your Sleep Health
If you are experiencing symptoms or concerns related to obstructive sleep apnea, seek professional support early. A qualified specialist can guide you through diagnosis, management, and long-term care options to help you sleep better and live healthier. Reach out today and begin your journey toward improved well-being.
● ABOUT DR ANAND SINGH
About Dr Anand Singh
Dr Anand Singh is a highly experienced Consultant Respiratory Physician with over a decade of experience in the field.
Dr Singh is a well known Chest Consultant and Sleep Consultant who provides personalised treatment plan.
Dr Anand Singh is a consultant Respiratory Physician at West Hertfordshire Teaching Hospitals NHS Trust
(Watford General and Hemel Hempstead Hospital where he leads the Sleep and Non-Invasive ventilation Service
and Respiratory High Dependency unit. He undertakes sub-speciality clinics in Interstitial Lung diseases
and Sleep Apnoea as well as conducting general respiratory medicine clinics.
Professional Memberships
Recommended by patients
Frequently Asked Questions
- What is the first step if I suspect sleep apnea?
The first step is to consult a qualified healthcare provider who can assess your symptoms and recommend whether you need a sleep study or further evaluation.
- Can lifestyle changes reduce OSA severity?
Yes. Weight loss, reducing alcohol intake, and improving sleep hygiene can help reduce the severity of obstructive sleep apnea in many adults.
- Is CPAP the only treatment available?
No. While CPAP is considered the most effective treatment, alternatives include oral appliances, positional therapy, hypoglossal nerve stimulation, and surgery in selected cases.
- Can untreated OSA lead to long-term health risks?
Yes. If left untreated, OSA can increase the risk of hypertension, diabetes, heart disease, mood changes, and difficulty concentrating.
- Are sleep studies necessary for diagnosis?
Yes. A sleep study is essential for accurate diagnosis. Those who are abroad or frequently traveling may also choose options like sleep apnea treatment in London for timely care and evaluation.
Specialist Assessment & Treatment by a Pulmonary Consultant
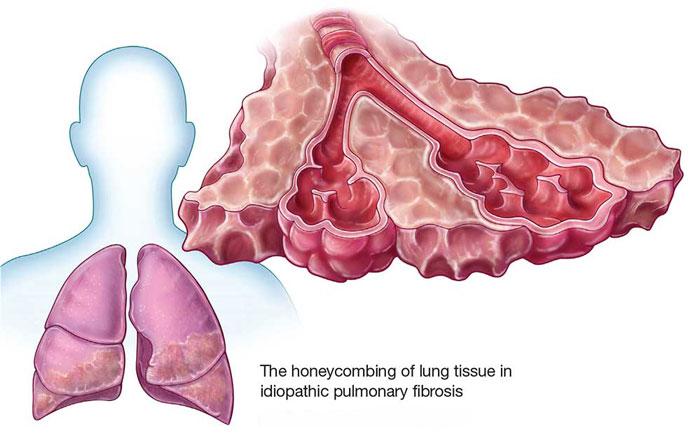
Pulmonary fibrosis is a progressive condition where the lungs develop scarring of the tissues, leading to breathing complications. An evaluation by an experienced pulmonary consultant is required as soon as possible to diagnose and provide management of the condition.
Chest and Sleep Doctor: Pulmonary fibrosis is considered and tackled by Dr Anand Singh, a consultant respiratory and pulmonary specialist, offering their services at Chest and Sleep Doctor, London.
Overview
Pulmonary fibrosis: This refers to lung thickening and stiffening as a result of scarring. Such conditions impact the lungs’ ability to diffuse oxygen from the lungs to the arteries.
Certain cases are referred to as idiopathic pulmonary fibrosis (IPF), where the cause is not well defined. This may also be related to exposure, autoimmune disease, drugs, and previous lung damage. The specific kind and severity of the disease are well defined after a thorough assessment by a pulmonary consultant
Symptoms
Common symptoms of pulmonary fibrosis include:
- Shortness of breath, particularly during physical activity
- Persistent dry cough
- Fatigue and reduced stamina
- Chest discomfort
- Gradual decline in exercise tolerance
If these symptoms persist, consultation with a pulmonologist doctor near me is recommended for early specialist assessment.
Diagnosis
Pulmonary fibrosis requires specialist assessment and cannot be diagnosed based on symptoms alone. Evaluation by a pulmonary consultant may include:
- Detailed medical history and physical examination
- Lung function tests
- High-resolution chest imaging
- Blood tests to assess possible underlying causes
Accurate diagnosis is essential to guide appropriate treatment and monitoring.
Treatment & Management
While pulmonary fibrosis cannot be reversed, specialist management can significantly slow the progression of the disease, reduce symptoms, and improve quality of life.
Management may include:
- Medication to control scarring and inflammation in the lungs
- Breathlessness management strategies
- Regular lung function follow-up
- Appropriate referral for pulmonary rehabilitation
All care is overseen by Dr Anand Singh, ensuring continuity with a dedicated pulmonary consultant.
Why See a Pulmonary Consultant?
Pulmonary fibrosis is a complex condition that benefits from specialist care. Seeing a pulmonary consultant ensures:
- Diagnosis and classification of diseases
- Access to appropriate investigations
- Individualized treatment planning
- Ongoing specialist follow-up
For patients looking for pulmonologists near me, having a private consultation is important because it gives patients access to specialist treatment on time.
When to Seek Specialist Advice
You should consider specialist assessment if you have:
- Worsening breathlessness
- Persistent respiratory symptoms
- Lung scarring found on imaging
- A previous diagnosis requiring ongoing specialist care
Early consultations with a pulmonologist doctor near me may help optimize treatments and outcomes.
Book an Appointment
If you are concerned about pulmonary fibrosis or ongoing breathing difficulties, specialist support is available. Private consultations in London. Appointments available without long waiting times
● ABOUT DR ANAND SINGH
About Dr Anand Singh
Dr Anand Singh is a highly experienced Consultant Respiratory Physician with over a decade of experience in the field.
Dr Singh is a well known Chest Consultant and Sleep Consultant who provides personalised treatment plan.
Dr Anand Singh is a consultant Respiratory Physician at West Hertfordshire Teaching Hospitals NHS Trust
(Watford General and Hemel Hempstead Hospital where he leads the Sleep and Non-Invasive ventilation Service
and Respiratory High Dependency unit. He undertakes sub-speciality clinics in Interstitial Lung diseases
and Sleep Apnoea as well as conducting general respiratory medicine clinics.
Professional Memberships
Recommended by patients
Frequently Asked Questions
1. What is pulmonary fibrosis?
Pulmonary fibrosis is an ongoing condition of the lungs wherein scars begin forming inside the lungs, and this causes breathing problems and inhibits the flow of oxygen in the blood.
2. What are the early signs of pulmonary fibrosis?
The early stages of this condition can give rise to symptoms such as breathing difficulties when exercising, a dry cough persisting in the respiratory tract, feeling tired, and experiencing reduced tolerance to exercise.
3. Do I need a referral to see a pulmonary consultant?
Referral is not required for a private consultation. You may also schedule an appointment directly with Dr. Anand Singh for evaluation and treatment of pulmonary fibrosis.
4. Can pulmonary fibrosis be treated?
Though there is no cure for this condition, it is possible to halt its progression. Based on the type of pulmonary fibrosis, the consultant pulmonologist creates the best possible treatment plan to help manage the situation.
5. What causes pulmonary fibrosis?
In some cases, the cause is unknown (idiopathic pulmonary fibrosis). Other causes may include environmental exposure, autoimmune conditions, certain medications, or previous lung injury.
6. How quickly should I see a specialist if pulmonary fibrosis is suspected?
Early specialty care evaluation is needed. If pulmonary fibrosis is a concern, a review of the case with a pulmonologist or a pulmonary specialist is important to ensure an accurate diagnosis and prompt management.
7. Will pulmonary fibrosis get worse over time?
Pulmonary fibrosis is a progressive condition; however, it may progress at a slow rate. It requires regular monitoring. Specialist treatment can also slow down the process.
8. What tests might be done during my consultation?
Your consultation may involve reviewing previous scans or tests and arranging lung function tests, imaging, or blood tests if required to confirm the diagnosis and guide treatment.
What is Bronchoscopy?
Bronchoscopy is a procedure used to evaluate the airways, lungs or lymph nodes in the chest for abnormalities and to treat conditions such as abnormal growths or foreign bodies causing airway obstruction.
Types
There are two types of bronchoscopes that may be used: Flexible and Rigid.
Flexible bronchoscopy uses a long, thin, flexible lighted tube that can access the small airway branches. A sample of tissue or a biopsy may be obtained through the bronchoscope for laboratory study.
Rigid bronchoscopy involves the use of a rigid, straight, hollow metal tube. Rigid bronchoscopy is indicated when the airway is obstructed by blood or foreign objects. This is usually done by Thoracic Surgeons .
Endobronchial Ultrasound is a special type of Camera test which uses Ultrasound guidance to sample Lymph nodes in the chest and Tumours in the Lungs .
Indications
Bronchoscopy is commonly performed to evaluate abnormal findings on a chest X-ray or CT scan and obtain wasings / biopsies for further studies. It may also be used to diagnose airway problems such as:
- A Persistent cough.
- Difficulty breathing.
- Blood in the sputum and.
- Lung cancer.
Pre-procedural preparation
Inform your doctor if you are pregnant or allergic to any medications. Other tests may also be ordered prior to the procedure. To reduce the risk of bleeding, you will have to discontinue taking blood thinning medications and non-steroidal anti-inflammatory drugs a few days before the procedure. You should abstain from food and drink after midnight before the procedure and if instructed to take medications, you should do so only with a sip of water.
Procedure
During a bronchoscopy, your blood pressure, oxygen level and heart rate are continually monitored.
Flexible bronchoscopy may be performed with you lying on your back or in a reclined or upright position. A sedative will be administered to help you relax and an intravenous line will be inserted for additional medications. A local anesthetic will be sprayed into your nose and mouth to reduce your gag reflex and minimize discomfort from insertion of the bronchoscope. In case of narrow nasal passages, the tube may be inserted through your mouth. The bronchoscope is gently inserted past the vocal cords and trachea into your lung while your doctor looks for abnormalities. Instruments are passed through the bronchoscope to obtain tissue and fluid samples or to perform other procedures. Your airway will then be washed with a saline solution.
A rigid bronchoscopy is performed under general anesthesia. Your neck is extended and the bronchoscope is gently inserted through your mouth and windpipe. Biopsy samples are obtained and the airway is washed with saline.
Post-Procedural Care
Following the procedure, you should avoid drinking or eating for at least 2 hours. Starting with small sips of water you can then gradually resume a normal diet. Avoid smoking for at least 24 hours after the procedure. You should not drive, drink alcohol or operate machinery for 24 hours after receiving the sedative. You may experience a sore throat which can be soothed by warm salt water gargles or throat lozenges. Consult your doctor immediately if you have breathing problems, persistent fever, or significant bleeding.
Risks and Complications
Bronchoscopy is generally a safe test but as with any procedure complications may occur and can include:
Tear in the lung or bleeding due to a biopsy instrument.
Breathing impairment.
Arrhythmias or irregular heart rhythms.
Infection such as pneumonia.
Hoarseness.
● ABOUT DR ANAND SINGH
About Dr Anand Singh
Dr Anand Singh is a highly experienced Consultant Respiratory Physician with over a decade of experience in the field.
Dr Singh is a well known Chest Consultant and Sleep Consultant who provides personalised treatment plan.
Dr Anand Singh is a consultant Respiratory Physician at West Hertfordshire Teaching Hospitals NHS Trust
(Watford General and Hemel Hempstead Hospital where he leads the Sleep and Non-Invasive ventilation Service
and Respiratory High Dependency unit. He undertakes sub-speciality clinics in Interstitial Lung diseases
and Sleep Apnoea as well as conducting general respiratory medicine clinics.
Professional Memberships
Recommended by patients
Lung function tests are a useful way of determining how well the lungs are working. They are an important tool to help identify the cause of breathlessness or lung disease. Lung function tests help to determine airflow, lung capacity and the ability of the lungs to exchange oxygen and carbon dioxide between the blood and lungs.
Tests carried out in the lung function laboratory include:
- Spirometry
- Body plethysmography
- Gas transfer
- Mouth pressures
- Fractional exhaled nitric oxide
- Hypoxic challenge (fitness to fly) test
- Cardiopulmonary exercise tests
Spirometry
Spirometry allows the determination of airflow limitation in the lungs. The individual will be asked to wear a clip on their nose that prevents air from escaping from the nose. Following a deep breath they are asked to blow out as quickly and as forcibly as they can into a mouth piece.
In addition to identifying airflow limitation in your airways spirometry allows determination of obstructive and restrictive lung disease. For example, to differentiate between asthma and COPD, or interstitial lung disease, or chest wall restriction.
Sometimes a bronchodilator such as salbutamol is administered and the spirometry test repeated 15 min later. This will allow to determine if their is significant dilatation of the airways. Significant bronchodilator reversibility as seen in asthma is an increase in forced expiratory volume in 1 second of 12% or more or more than 200 mL.
Body plethysmography
Body plethysmography is a test used to determine lung volumes. For example, it can determine your total lung capacity (ie. how much total amount of air in the lungs at the end of full inspiration) and the residual volume (ie. the total amount of air in the lungs at the end of full expiration). People with restrictive lung disease have reduced lung volumes and those with obstructive lung disease may have a increased residual volume because narrow airways cause air to be trapped in the lungs as it isn’t completely exhaled.
Gas transfer
This tests is also known as transfer factor or diffusing capacity. It is a measure of how well the lungs exchange gases between themselves and the blood. To do this test a mixture containing a small amount of helium and carbon monoxide is inhaled through a deep breathe. After a breath hold of 8 to 10 seconds the air from the lungs is slowly exhaled into the machine for a reading. To get an accurate representation the value obtained needs to be corrected for the lung volume and the haemoglobin in blood as these two parameters affect the transfer factor value. A low transfer factor indicates impaired gas exchange.
Respiratory muscle tests
Respiratory muscle tests are useful to determine if the breathing problem is due to weak respiratory muscles. These tests include:
Mouth pressures
After breathing our air from the lungs as long as possible the person is asked to suck hard on a mouthpiece for 1 second to measure the maximal inspiratory pressure. Then after taking a deep breath in the person exhales forcibly against a closed off mouthpiece to determine the maximal expiratory pressure.
Sniff pressures
A small probe is inserted into one nostril and measures the inspiratory and expiratory pressures when the person sniffs.
Lying and sitting / standing vital capacity
Spirometry is done lying down in the supine position and then again in a sitting or standing position. A significant reduction in the supine VC may suggest respiratory muscle and diaphragmatic weakness.
Fractional exhaled nitric oxide
Inflammation in the lungs can produce nitric oxide and high levels of NO (>40 ppb) may suggest asthma. However not all types of asthma will produce a high level of NO. This test involves taking in a deep breath and then slowly exhaling at a constant rate into the machine that takes the reading.
Fitness to fly test
This test mimics the conditions in a pressurised cabin at altitude. Although an airplane may be flying at higher altitude the cabin is pressurised to 5000 – 8000 feet where the oxygen concentration in air is reduced from 21% to 15%. For people with healthy lungs and oxygen saturations >94% this isn’t a problem. But for people with signifcant respiratory disease and oxygen saturations >95% there oxygen saturations may drop significantly during the flight leading to respiratory distress.
To do the test the person sits in a cabin breathing air with 15% oxygen and using a pulse oximeter the oxygen saturation is monitored and is used to determine if the person needs oxygen during a flight, and if they do, how much oxygen per minute they will need.
Cardiopulmonary exercise test
● ABOUT DR ANAND SINGH
About Dr Anand Singh
Dr Anand Singh is a highly experienced Consultant Respiratory Physician with over a decade of experience in the field.
Dr Singh is a well known Chest Consultant and Sleep Consultant who provides personalised treatment plan.
Dr Anand Singh is a consultant Respiratory Physician at West Hertfordshire Teaching Hospitals NHS Trust
(Watford General and Hemel Hempstead Hospital where he leads the Sleep and Non-Invasive ventilation Service
and Respiratory High Dependency unit. He undertakes sub-speciality clinics in Interstitial Lung diseases
and Sleep Apnoea as well as conducting general respiratory medicine clinics.
Professional Memberships
Recommended by patients
Radiological imaging is very useful in visualising the chest and lungs to establish a diagnosis.
Commonly used radiological imaging includes:
- Chest x-ray
- Computed Tomography (CT)
- Pleural / Thoracic Ultrasound
- Positron Emission Tomography (PET)
- Magnetic Resonance Imaging (MRI)
- Ventilation – Perfusion (VQ) scans
Chest x-ray
Chest x-rays can be obtained quickly and offer a rapid general view of the lungs to make an initial diagnosis or determine progress after treatment.
The radiation from a chest x-ray is 0.02 mSV and is equivalent to 5 days of background radiation.
CT scans
CT scans offer a more detailed view of the chest including the heart, blood vessels, lymph nodes, airways, lung tissue and chest wall. Usually the test takes only a few seconds. Sometimes a dye (contrast) is injected to better help visualise specific structures and scans taken before and after injection of dye. For example, injection of dye and scanning whilst the dye is in the pulmonary arteries allows the detection of clots (emboli) within the pulmonary arteries. On other occasions scans need to be taken during inspiration and expiration to help in identifying specific airways disease.
Regarding the contrast, it is important that you let Dr. Singh and Radiology department of Hospital know if you are allergic to contrast
A CT scan delivers approximately 6.1 mSV of radiation that is equivalent to 2 years of background radiation. However, in some cases, for example with lung cancer screening, low dose CT scans can be done, which reduce the radiation dose to 1.5 mSV.
Thoracic / Pleural Ultrasound
This involves no radiation . The Use of Ultrasound helps detect presence of fluid in the chest cavity / pleura and estimate its size . It also helps guide the procedure to remove fluid from the chest.
PET CT scans
PET CT scans are nuclear medicine scans where a nuclear dye is injected to demonstrate areas of the body that are more active. They imaging is combined with CT scans to offer 3D visualisation of the body and is particularly useful to detect active sights of inflammation, infection and cancer.
The scan is safe but pregnant woman should only have it in an emergency. The scan delivers approximately 22 mSV of radiation that is equivalent to 3 years of background radiation. Drinking plenty of water after the scan helps to flush the body of the radioactive tracer. As a precaution you should avoid coming in to close contact with pregnant woman and young children for 6 hours.
Ventilation-Perfusion scans
These scans use radioactive tracer to detect ventilation (airflow) and perfusion (blood flow) in the lungs. This allows detection of areas where there is a problem with ventilation or perfusion and helps make a diagnosis of pulmonary emboli (blood clots in the lungs). As the test is done in two parts it can take up to 30 min to complete.
Ventilation-Perfusion scans can be combined with CT using single-photon emission computed tomography (SPECT) to provide 3D information, with lower dose of radiation that with a CT pulmonary angiogram, and avoiding the use the contrast
This is often the investigation of choice to detect blood clots in the lungs of pregnant woman, using only the radioactive tracer to detect perfusion, as CT pulmonary angiogram delivers a higher dose of radiation to the breast tissue of pregnant woman.
● ABOUT DR ANAND SINGH
About Dr Anand Singh
Dr Anand Singh is a highly experienced Consultant Respiratory Physician with over a decade of experience in the field.
Dr Singh is a well known Chest Consultant and Sleep Consultant who provides personalised treatment plan.
Dr Anand Singh is a consultant Respiratory Physician at West Hertfordshire Teaching Hospitals NHS Trust
(Watford General and Hemel Hempstead Hospital where he leads the Sleep and Non-Invasive ventilation Service
and Respiratory High Dependency unit. He undertakes sub-speciality clinics in Interstitial Lung diseases
and Sleep Apnoea as well as conducting general respiratory medicine clinics.
Professional Memberships
Recommended by patients
Blood tests are used to rapidly get information about your general health. They are also essential for the diagnosis of suspected medical conditions. For example, for the identification of immunodeficiency or causes of bronchiectasis.
Based on the information obtained during your consultation Dr. Anand Singh will discuss with you the blood that should be done.
Blood tests can be taken at all clinic location sites at the time of your consultation or when attending for other investigations. If there are special requirements for more specialist tests then Dr. Anand Singh will make you aware of these.
List of common tests
- Full blood count
- IGE Rast Panel to test for Allergies especially when Asthma is suspected
- Auto immune blood screen when Interstitial Lung disease in suspected or confirmed
- Kidney function
- Liver function
- Thyroid function
- C-reactive protein
- D-Dimer
- Brain Natriuretic peptide
- High sensitivity troponin
- Alpha-1-anti-trypsin level
- Serum immunoglobulin levels
- Serum ACE levels to evaluate for Sarcoidosis
- Serum Interferon Gamma Release Assay (IGRA )tests if Tb is suspected
Other tests
On a case by case basis other blood tests may sometimes be required
● ABOUT DR ANAND SINGH
About Dr Anand Singh
Dr Anand Singh is a highly experienced Consultant Respiratory Physician with over a decade of experience in the field.
Dr Singh is a well known Chest Consultant and Sleep Consultant who provides personalised treatment plan.
Dr Anand Singh is a consultant Respiratory Physician at West Hertfordshire Teaching Hospitals NHS Trust
(Watford General and Hemel Hempstead Hospital where he leads the Sleep and Non-Invasive ventilation Service
and Respiratory High Dependency unit. He undertakes sub-speciality clinics in Interstitial Lung diseases
and Sleep Apnoea as well as conducting general respiratory medicine clinics.
Professional Memberships
Recommended by patients